Physical Changes of Late Adulthood
Age sixty-five is considered a milestone and the beginning of late adulthood. Reaching this age generally brings about retirement from work, eligibility for Social Security and Medicare benefits, income tax advantages, reduced fares and admission prices to leisure events, and special purchase or discount privileges.
It is projected that by the year 2020, approximately 16.5% of the population will be sixty-five years of age or older (up from 4.1% in 1900, 8.1% in 1950, and 12.4% in 2000) (Himes, 2001). This percentage is expected to increase to 20.8% by 2060.
It is projected that by the year 2020, approximately 16.5% of the population will be sixty-five years of age or older (up from 4.1% in 1900, 8.1% in 1950, and 12.4% in 2000) (Himes, 2001). This percentage is expected to increase to 20.8% by 2060.
- Changes in body systems and organs with age are highly variable and may be results of disease, which in turn may be affected by lifestyle.
- Most body systems generally continue to function fairly well, but the heart becomes more susceptible to disease. Reserve capacity declines.
- Although the brain changes with age, the changes are usually modest. They include loss or shrinkage of nerve cells and a general slowing of responses. However, the brain also seems able to grow new neurons and build new connections late in life.
- Visual and hearing problems may interfere with daily life but often can be corrected. Irreversible damage may result from age-related macular degeneration or glaucoma. Losses in taste and smell may lead to poor nutrition. Training can improve muscular strength, balance, and reaction time. Older adults tend to be susceptible to accidents and falls.
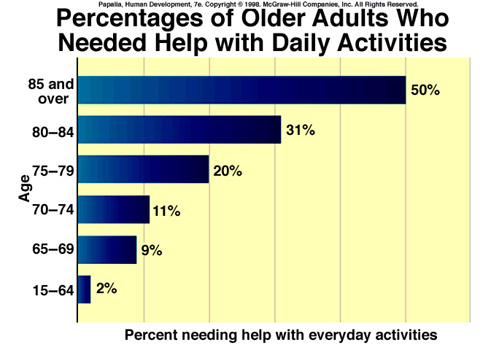
- Most older people are reasonably healthy, especially if they follow a healthy lifestyle. Most do have chronic conditions, but these usually do not greatly limit activities or interfere with daily life. The proportion of older adults with physical disabilities has declined. Still, older adults do need more medical care than younger ones.
- Exercise and diet are important influences on health. Loss of teeth can seriously affect nutrition.
|
|
Quick Facts
Primary Changes
* The universal & irreversible physical changes that occur to living creatures, as they grow older is called primary aging.
* Every part of the body slows down, from speech to heart rate, from speed of walking to speed of thinking, from reaction time to reading time.
* Every body system also becomes less efficient with age, with a gradual reduction in capacity and organ reserve.
* Appearance changes as aging occurs, such things as skin, hair, body height, body shape, and body weight.
* The skin is often the first sign: It becomes drier, thinner, and less elastic; wrinkles and visible blood vessels and pockets of fat appear.
* The hair also undergoes obvious changes, growing thinner and grayer and, in many people, eventually becoming white or disappearing completely.
* Most older people are more than an inch shorter than they were in early adulthood, because the vertebrae begin settling closer together in middle age.
* Body shape is affected by redistribution of fat, disappearing from the arms, legs, and upper face and collecting in the torso and the lower face.
* Older adults often weigh less than they did at age 50 or so, partly because of a reduction in muscle tissue, which is relatively dense and heavy. * The difference in weight tends to be more noticeable in men than in women, because men have relatively more muscle and less body fat. * Another reason older people weigh less is a loss of bone calcium, which makes bones more porous and fragile. * Please note that weight reduction is usually not good
*Although only 10 percent of the aged see well without corrective lenses, another 80 percent can see quite well with glasses and the remaining 10 percent have series vision problems. * Cataracts is a common eye disease among the elderly involving a thickening of the lens; it can cause distorted vision if left untreated.
* Glaucoma is a disease of the eye that can destroy vision if left untreated. It involves hardening of the eyeball due to a fluid buildup within the eye.
* Senile macular degeneration is deterioration of the retina that affects one in twenty-five people between the ages of 66 and 74 and one in six of those age 75 and older. This condition is hard to treat medically and is therefore the leading cause of legal blindness.
* Presbycusis is the age-related hearing loss that affects about 40 percent of those aged 65 or older. * Most often presbycusis can be remedied with hearing aids. * Tinnitis - buzzing or rhythmic ringing in the ears experienced by 10 percent of the elderly. The only treatment at the moment is surgery, which is not always successful. * The hard-of-hearing is likely to withdraw socially and to suspect that inaudible conversations are about them.
* The universal & irreversible physical changes that occur to living creatures, as they grow older is called primary aging.
* Every part of the body slows down, from speech to heart rate, from speed of walking to speed of thinking, from reaction time to reading time.
* Every body system also becomes less efficient with age, with a gradual reduction in capacity and organ reserve.
* Appearance changes as aging occurs, such things as skin, hair, body height, body shape, and body weight.
* The skin is often the first sign: It becomes drier, thinner, and less elastic; wrinkles and visible blood vessels and pockets of fat appear.
* The hair also undergoes obvious changes, growing thinner and grayer and, in many people, eventually becoming white or disappearing completely.
* Most older people are more than an inch shorter than they were in early adulthood, because the vertebrae begin settling closer together in middle age.
* Body shape is affected by redistribution of fat, disappearing from the arms, legs, and upper face and collecting in the torso and the lower face.
* Older adults often weigh less than they did at age 50 or so, partly because of a reduction in muscle tissue, which is relatively dense and heavy. * The difference in weight tends to be more noticeable in men than in women, because men have relatively more muscle and less body fat. * Another reason older people weigh less is a loss of bone calcium, which makes bones more porous and fragile. * Please note that weight reduction is usually not good
*Although only 10 percent of the aged see well without corrective lenses, another 80 percent can see quite well with glasses and the remaining 10 percent have series vision problems. * Cataracts is a common eye disease among the elderly involving a thickening of the lens; it can cause distorted vision if left untreated.
* Glaucoma is a disease of the eye that can destroy vision if left untreated. It involves hardening of the eyeball due to a fluid buildup within the eye.
* Senile macular degeneration is deterioration of the retina that affects one in twenty-five people between the ages of 66 and 74 and one in six of those age 75 and older. This condition is hard to treat medically and is therefore the leading cause of legal blindness.
* Presbycusis is the age-related hearing loss that affects about 40 percent of those aged 65 or older. * Most often presbycusis can be remedied with hearing aids. * Tinnitis - buzzing or rhythmic ringing in the ears experienced by 10 percent of the elderly. The only treatment at the moment is surgery, which is not always successful. * The hard-of-hearing is likely to withdraw socially and to suspect that inaudible conversations are about them.
Physical Development

The vast majority of physical changes observed during late adulthood are closely related to the process of advanced aging. Physical functioning and daily activities are curtailed as the organ systems degenerate. Many of the symptoms of organ degeneration appear promi- nently in middle adulthood, but they become even more pronounced as people progress through late adulthood.
The aging process in late adulthood is termed senescence. The general effects of aging combine to make the body’s organ systems work less efficiently. For quite a while, people can compensate for the declining efficiency of their organs and the body in general, but the decline becomes dramatic later in this stage.
The aging process in late adulthood is termed senescence. The general effects of aging combine to make the body’s organ systems work less efficiently. For quite a while, people can compensate for the declining efficiency of their organs and the body in general, but the decline becomes dramatic later in this stage.
Changes in Weight & Height
The loss of weight in men that begins in middle adulthood continues through late adult- hood. Elderly women begin to lose weight in gradual increments during this stage. Decreasing physical activity, less food consumption, lower metabolism, poorer health, and related factors result in a reduction of muscle and tissue mass and hence weight.
Reductions in weight also continue into late adulthood for both men and women (Abra- ham, 1979; Hegner, 1991). This loss in height is caused by compression of the spinal column and the softening of muscle and bone tissue. The changes also result in the characteristically stooped posture, with the head held forward and down from the body, seen in older people.
Reductions in weight also continue into late adulthood for both men and women (Abra- ham, 1979; Hegner, 1991). This loss in height is caused by compression of the spinal column and the softening of muscle and bone tissue. The changes also result in the characteristically stooped posture, with the head held forward and down from the body, seen in older people.

|


|
Teeth
Total loss of teeth occurs in a sizable minority of people between the ages of sixty-five and seventy-four. Advanced age is asso- ciated with a higher incidence of periodontal disease and gingivitis, inflammations of gum tissue that contribute highly to tooth loss. Many of the dental problems of old age, however, are the result of earlier neglect.
Dental problems contribute to poor eating habits that lead to malnutrition. Some eld- erly people do not get dentures to replace missing teeth for financial reasons; others have poorly fitting dentures. As a result, they may eat only foods that are easy to chew, eliminat- ing many vegetables, fruits, and meats from their diet.
Muscular & Skeletal System
The ability to move about becomes more restricted as aging advances because of changes in muscle and bone functioning. Muscles atrophy, reducing strength and restricting movement. Loss of elasticity in muscle tissue reduces flexibility, causing stiffness. Osteoporosis leads to easier bone breakage, kyphosis (“humpback” posture), and scoliosis (S-curved spinal column). Back pain increases in frequency and intensity, reflecting deterioration of the vertebrae
Arthritis and rheumatism are the most prevalent musculoskeletal dis- orders among the elderly. Other con- ditions that often cause disability or discomfort at this stage are muscle cramps, bursitis in the shoulder or elbow, and gout (a metabolic disor- der that results from uric acid crys- tals forming at joint areas, especially in the feet).
Arthritis and rheumatism are the most prevalent musculoskeletal dis- orders among the elderly. Other con- ditions that often cause disability or discomfort at this stage are muscle cramps, bursitis in the shoulder or elbow, and gout (a metabolic disor- der that results from uric acid crys- tals forming at joint areas, especially in the feet).

Cardiovascular System

The effects of aging on the heart and blood vessels that became increasingly apparent in middle
adulthood worsen in late adulthood.There is further accumulation of fatty material in the heart muscle and in the arteries (atherosclerosis), the heart valves thicken, and arterioscle- restricted. rosis (hardening of the arteries)
becomes more pronounced (Schrier, 1990; Spence & Mason, 1987). These conditions cause higher blood pressure, extra stress on the heart, and related cardiovascular problems, although regular exercise has been found to be beneficial in maintaining cardiovascular responsiveness (Thompson, Crist & Osborn, 1990; Van camp & Boyer, 1989).
Decreased cardiac output further jeopardizes the health and well-being of the elderly (Spence & Mason, 1987). The slower heart rate of older people results in a decreased level of oxygen in the blood, which is why elderly people tire more easily and cannot endure stress as well as younger people.
Coronary heart disease increases steadily during late adulthood. It is a leading cause of death at this stage of life. Coronary heart disease stems from a diminished supply of oxy- gen to the heart muscle through the blood caused by hypertension, atherosclerosis, or coronary aneurysm (ruptured blood vessel in the heart muscle). Over a long period of time, it can lead to heart attack or congestive heart failure.
adulthood worsen in late adulthood.There is further accumulation of fatty material in the heart muscle and in the arteries (atherosclerosis), the heart valves thicken, and arterioscle- restricted. rosis (hardening of the arteries)
becomes more pronounced (Schrier, 1990; Spence & Mason, 1987). These conditions cause higher blood pressure, extra stress on the heart, and related cardiovascular problems, although regular exercise has been found to be beneficial in maintaining cardiovascular responsiveness (Thompson, Crist & Osborn, 1990; Van camp & Boyer, 1989).
Decreased cardiac output further jeopardizes the health and well-being of the elderly (Spence & Mason, 1987). The slower heart rate of older people results in a decreased level of oxygen in the blood, which is why elderly people tire more easily and cannot endure stress as well as younger people.
Coronary heart disease increases steadily during late adulthood. It is a leading cause of death at this stage of life. Coronary heart disease stems from a diminished supply of oxy- gen to the heart muscle through the blood caused by hypertension, atherosclerosis, or coronary aneurysm (ruptured blood vessel in the heart muscle). Over a long period of time, it can lead to heart attack or congestive heart failure.
Respiratory System

The lungs have lowered capacity for inhaling and exhaling air in late adulthood (Horan & Brouwer, 1990; Spence & Mason, 1987). There are three causes of this reduced capacity. First, a change in collagen composition of the lungs causes them to become less elastic and thus less capable of expanding and contract- ing. Second, the diaphragm and chest muscles that help expand and contract the chest weaken. Third, age-related conditions such as scoliosis reduce chest capacity.
Among the most common serious respiratory conditions among the elderly are cancer of the lungs, emphysema, and pneumonia. Lung cancer increases considerably during late adulthood; it is associated with chronic conditions such as smoking, pollution, and occupa- tional hazards. Emphysema is a condition involving destruction of lung tissue that results in lowered lung elasticity. People with emphysema have difficulty breathing and moving about freely. Pneumonia is an inflammation of the lungs. It increases in incidence in old age because of decreased lung efficiency, poor circulation, and lowered resistance to infection. Pneumonia is a particular risk for an elderly person who is bedridden for an extended period of time because physical inactivity prevents the lungs from clearing themselves.
Among the most common serious respiratory conditions among the elderly are cancer of the lungs, emphysema, and pneumonia. Lung cancer increases considerably during late adulthood; it is associated with chronic conditions such as smoking, pollution, and occupa- tional hazards. Emphysema is a condition involving destruction of lung tissue that results in lowered lung elasticity. People with emphysema have difficulty breathing and moving about freely. Pneumonia is an inflammation of the lungs. It increases in incidence in old age because of decreased lung efficiency, poor circulation, and lowered resistance to infection. Pneumonia is a particular risk for an elderly person who is bedridden for an extended period of time because physical inactivity prevents the lungs from clearing themselves.
Digestive System
Digestive problems generally increase through adulthood (Spence & Mason, 1987). In old age, the most commonly reported digestive disorders are constipation, hernia, gallbladder conditions, gastritis (heartburn), and diverticulitis (Drury & Howie, 1979; Whitehead, Drinkwater & Cheskin, 1989).
Constipation and hemorrhoids are frequent complaints of the elderly. Their concern with not having a regular daily bowel movement may be more of a matter of socialization than a true effect of aging, however. Of greater concern for many elderly individuals is the high rate of hemorrhoids and the reliance on laxatives to produce regular bowel move- ments. This often is related more to dietary practices than to the aging process as well. These conditions may be controlled by adding more fiber to the diet in the form of grain bran, fresh fruits, vegetables, and nuts or by taking dietary supplements containing fiber (Hazard, 1990). In general, between twenty and thirty grams of dietary fiber should be consumed by adults daily for effective control of constipation and hemorrhoids.
Hiatal hernia, a condition in which a portion of the stomach slides up next to the esophagus, is common among the elderly, especially among overweight or obese individu- als. Hiatal hernia causes indigestion, gastritis, chest pain, and difficulty in swallowing. It can be treated with therapeutic methods or surgery if severe.
Diverticulitis is an inflammation of a portion of an intestine that causes pain, nausea, and a change in bowel habits. It is usually treated without surgery, unless the affected area of the intestine perforates or ruptures.
Gallbladder problems in old age usually involve gallstones or inflammation of the gall- bladder. The gallbladder stores bile from the liver. Gallstones sometimes form from insolu- ble substances in the bile. They don’t cause serious problems unless they block the duct leading from the gallbladder to the intestine. “Gallbladder attacks” are very painful, how- ever, and may be accompanied by nausea and vomiting.
Constipation and hemorrhoids are frequent complaints of the elderly. Their concern with not having a regular daily bowel movement may be more of a matter of socialization than a true effect of aging, however. Of greater concern for many elderly individuals is the high rate of hemorrhoids and the reliance on laxatives to produce regular bowel move- ments. This often is related more to dietary practices than to the aging process as well. These conditions may be controlled by adding more fiber to the diet in the form of grain bran, fresh fruits, vegetables, and nuts or by taking dietary supplements containing fiber (Hazard, 1990). In general, between twenty and thirty grams of dietary fiber should be consumed by adults daily for effective control of constipation and hemorrhoids.
Hiatal hernia, a condition in which a portion of the stomach slides up next to the esophagus, is common among the elderly, especially among overweight or obese individu- als. Hiatal hernia causes indigestion, gastritis, chest pain, and difficulty in swallowing. It can be treated with therapeutic methods or surgery if severe.
Diverticulitis is an inflammation of a portion of an intestine that causes pain, nausea, and a change in bowel habits. It is usually treated without surgery, unless the affected area of the intestine perforates or ruptures.
Gallbladder problems in old age usually involve gallstones or inflammation of the gall- bladder. The gallbladder stores bile from the liver. Gallstones sometimes form from insolu- ble substances in the bile. They don’t cause serious problems unless they block the duct leading from the gallbladder to the intestine. “Gallbladder attacks” are very painful, how- ever, and may be accompanied by nausea and vomiting.
|

|
Genitourinary System

Elderly people are susceptible to a variety of dis- orders in the reproductive organs and the urinary system (kidneys, bladder, and urethra) (Schrier, 1990; Spence & Mason, 1987). As people age, there is a decrease in the blood flow through the kidneys as well as a gradual decrease in the kidneys’ efficiency to remove wastes from the blood. Among people of advanced age, urinary incontinence (the inabil- ity to retain urine in the bladder until voluntarily released) is a very real and embarrassing problem (Ruff & Reaves, 1989).
These changes bring on certain conditions that affect the functioning of the urinary system. Men commonly experience enlargement of the prostate gland, which causes blockage of the urine flow. This encourages bladder infections and other complications. The most common types of cancer affecting this system in elderly men are cancer of the bladder and of the prostate gland.
Women have more urinary system problems than men throughout life. Bladder infec- tions, such as cystitis, are frequent. In late adulthood, women are at increased risk for prob- lems of the vaginal area, prolapsed uterus, and cancer of the cervix, vulva, and breasts. Breast cancer is a leading cause of death among elderly women (U.S. Bureau of the Census, 2000).
These changes bring on certain conditions that affect the functioning of the urinary system. Men commonly experience enlargement of the prostate gland, which causes blockage of the urine flow. This encourages bladder infections and other complications. The most common types of cancer affecting this system in elderly men are cancer of the bladder and of the prostate gland.
Women have more urinary system problems than men throughout life. Bladder infec- tions, such as cystitis, are frequent. In late adulthood, women are at increased risk for prob- lems of the vaginal area, prolapsed uterus, and cancer of the cervix, vulva, and breasts. Breast cancer is a leading cause of death among elderly women (U.S. Bureau of the Census, 2000).
Brain & Nervous System
Several developmental changes in the brain and central nervous system are related to advanced aging (Albert & Killiany, 2001; Spence & Mason, 1987; Vinters, 2001). First, the speed of nerve cell transmission slows with age. Second, brain and nerve cells diminish in number. These two factors, plus decreased transmission of oxygen to the brain, produce the slowing in reaction time that is commonly observed among elderly individuals.
Reaction time affects perception and memory as well as the soundness of various reflexes. Progressively slower reaction times endanger the safety of the elderly people, especially when they are driving. Many states now require extra testing for issuance of driver’s licenses to the elderly.
Reduced availability of oxygen to the brain can contribute to other conditions that are troublesome to elderly individuals. Sleep disturbances, memory difficulties, and general irritability are related to decreased cerebral blood flow and to changes in the biochemical functioning of the brain in old age (Pollak, Perlick & Linsner, 1990). Insomnia is a fre- quent complaint among the elderly (Cassel, 1990). There is a general trend to need less sleep as age increases. A newborn infant may sleep about sixteen hours daily, whereas school-age children sleep about ten hours, and adults about eight. Elderly people may be able to sleep only five hours or so a night.
Reaction time affects perception and memory as well as the soundness of various reflexes. Progressively slower reaction times endanger the safety of the elderly people, especially when they are driving. Many states now require extra testing for issuance of driver’s licenses to the elderly.
Reduced availability of oxygen to the brain can contribute to other conditions that are troublesome to elderly individuals. Sleep disturbances, memory difficulties, and general irritability are related to decreased cerebral blood flow and to changes in the biochemical functioning of the brain in old age (Pollak, Perlick & Linsner, 1990). Insomnia is a fre- quent complaint among the elderly (Cassel, 1990). There is a general trend to need less sleep as age increases. A newborn infant may sleep about sixteen hours daily, whereas school-age children sleep about ten hours, and adults about eight. Elderly people may be able to sleep only five hours or so a night.
CHANGES IN SENSATION, PERCEPTION, AND MOTOR SKILLS
The ability to adjust and adapt in late adulthood partly depends on the capacity to receive and process information gained through the senses. Elderly people experience sensory deprivation as the sensory organs and the area of the brain that regulate them decline in efficiency. This deprivation has enormous implications for mental alertness and contact with reality.

Vision
Age-related changes in vision during late adulthood include an increase in the threshold of light needed to stimulate retinal cells; a decrease in acuity (sharpness of vision) due to changes in the lens, pupil size, and accommodation (focusing ability); and a decrease in adaptation to dark and light environments (Fozard & Gordon-Salant, 2001; Saxon & Etten, 1978; Spence & Mason, 1987).
Elderly people can expect to experience several eye disorders that can limit visual abil- ity: “specks” in a visual field due to loose cells floating within the vitreous humor of the eyeballs; cataracts; glaucoma; macular degeneration, or a decreased blood supply to the retina, causing loss of visual sharpness when looking directly ahead but not in the periph- eral vision areas; and drooping eyelids. The risk of blindness increases considerably after age sixty, often because of glaucoma.
Age-related changes in vision during late adulthood include an increase in the threshold of light needed to stimulate retinal cells; a decrease in acuity (sharpness of vision) due to changes in the lens, pupil size, and accommodation (focusing ability); and a decrease in adaptation to dark and light environments (Fozard & Gordon-Salant, 2001; Saxon & Etten, 1978; Spence & Mason, 1987).
Elderly people can expect to experience several eye disorders that can limit visual abil- ity: “specks” in a visual field due to loose cells floating within the vitreous humor of the eyeballs; cataracts; glaucoma; macular degeneration, or a decreased blood supply to the retina, causing loss of visual sharpness when looking directly ahead but not in the periph- eral vision areas; and drooping eyelids. The risk of blindness increases considerably after age sixty, often because of glaucoma.

Hearing
Perhaps the most significant sensory change during late adulthood is hearing loss. It sometimes leads to a complete withdrawal from social interaction. Hearing handicaps increase considerably with age (Rowland, 1980; Spence & Mason, 1987). About half of all people older than sixty-five have some hearing loss. These losses occur earlier in men than women, perhaps because men were more likely to be exposed to hazardous noise on the job.
The loss of hearing for high-frequency sounds that was first noticed during middle adulthood continues. Loss of hearing in the mid to low-range frequencies becomes more likely with age. Many elderly people become deaf because of damage to the cochlea hair cells, hardening of the bones, and nerve damage to the structures of the inner ear that transmit sound waves to the brain (Fozard & Gordon-Salant, 2001).
Perhaps the most significant sensory change during late adulthood is hearing loss. It sometimes leads to a complete withdrawal from social interaction. Hearing handicaps increase considerably with age (Rowland, 1980; Spence & Mason, 1987). About half of all people older than sixty-five have some hearing loss. These losses occur earlier in men than women, perhaps because men were more likely to be exposed to hazardous noise on the job.
The loss of hearing for high-frequency sounds that was first noticed during middle adulthood continues. Loss of hearing in the mid to low-range frequencies becomes more likely with age. Many elderly people become deaf because of damage to the cochlea hair cells, hardening of the bones, and nerve damage to the structures of the inner ear that transmit sound waves to the brain (Fozard & Gordon-Salant, 2001).

Taste and smell
Taste and smell perception decline in old age. Many elderly people remark that food tastes bland, and season it heavily with salt, pepper, and other condi- ments to improve its flavor. This loss of taste is attributed to a decrease in the number of taste buds and to the need for stronger stimulation to taste receptors in the mouth. People do not smell odors as well in late adulthood. This is because of a decrease in the number of nerve fibers in the nose (Saxon & Etten, 1978; Spence & Mason, 1987). This decline has important safety implications. Elderly people sometimes cannot easily smell food that has burned during cooking or smoke from a house fire.
Taste and smell perception decline in old age. Many elderly people remark that food tastes bland, and season it heavily with salt, pepper, and other condi- ments to improve its flavor. This loss of taste is attributed to a decrease in the number of taste buds and to the need for stronger stimulation to taste receptors in the mouth. People do not smell odors as well in late adulthood. This is because of a decrease in the number of nerve fibers in the nose (Saxon & Etten, 1978; Spence & Mason, 1987). This decline has important safety implications. Elderly people sometimes cannot easily smell food that has burned during cooking or smoke from a house fire.
